Reactions to insect bites are painful conditions that develop due to the body's sensitivity to components of the poison or saliva that enter the body during bites. They can be allergic and toxic and in some cases can cause death. Every 10th inhabitant of our planet suffers from allergies to insect bites; Particularly dangerous in this regard is the venom of hymenoptera insects, which can initiate the development of anaphylaxis and lead to death.
The Allergology Department of CELT offers treatment for a child’s or adult’s reaction to insect bites in Moscow. Our multidisciplinary clinic employs leading domestic specialists who have modern diagnostic and treatment facilities and practice modern methods for eliminating allergic and toxic reactions. You can make an appointment with them online or by contacting our operators: +7 (495) 788-33-88
At CELT you can get advice from an allergist.
- Initial consultation – 3,500
- Repeated consultation – 2,300
Make an appointment
Causes of pneumonia
Viruses or bacteria are responsible for most cases of pneumonia (in children and adolescents, the infection is often caused by mycoplasma). The disease is also common in people suffering from gastroesophageal reflux. Inflammatory exudate occurs when food enters the lungs. Pneumonia can also be a complication of an upper respiratory tract infection or other infectious disease. Pneumonia can also be caused by fungi (candied pneumonia) and inhalation of allergic or chemical substances.
Who gets pneumonia more often?
There are factors that increase your chance of getting pneumonia. These include viral respiratory tract infections, congenital respiratory defects, old age, heart failure, diabetes and immunological problems.
The following groups of people are at high risk of developing pneumonia:
- people suffering from allergies;
- malnourished people;
- people who smoke or are exposed to tobacco smoke;
- people with weakened immune systems;
- people with congenital defects of the respiratory and circulatory systems.
Diagnosis of reactions to insect bites
The main task of an allergist who makes a diagnosis is to conduct a full medical history, which will allow you to establish the following:
- Previously noted reactions to insect bites;
- The presence of a bite by Hymenoptera;
- What kind of insect bit the patient?
In addition, an examination is carried out, as well as additional diagnostic studies aimed at identifying reactions in the form of disruption of systems and internal organs. They may be as follows:
- Ultrasound scanning of the peritoneal organs;
- Electrocardiography;
- Allergy tests.
Types of pneumonia
Doctors divide pneumonia into:
- bacterial;
- fungal;
- viral (often found in children over 5 years of age);
- allergic;
- chemical;
- typical;
- atypical;
- Also worth mentioning is an idiopathic pneumonia called idiopathic interstitial pneumonia. In this case, inflammation turns into fibrosis. Each type of pneumonia occurs differently. In some cases, the disease is asymptomatic, then we are talking about asymptomatic pneumonia.
Another division of pneumonia is distinguished:
- lobar pneumonia (includes one lobe and pleura);
- bronchopneumonia (germs penetrate the bronchi);
- segmental pneumonia.
Pneumonia according to ICD-10 classification
In the International Statistical Classification of Diseases and Related Health Problems (ICD-10), pneumonia is designated J12-J18.
- J12 - previously unclassified pneumonia, most often of viral origin;
- J13 - pneumonia caused by streptococci;
- J14 - pneumonia as a result of infection with bacteria H. influenzae;
- J15 - previously unclassified bacterial pneumonia;
- J16 - pneumonia caused by microorganisms not recommended by other types;
- J17 - pneumonia in previously classified diseases;
- J18 - pneumonia caused by unspecified microorganisms.
Patient characteristics
The present study involved 1587 children (965 boys, 622 girls) from 1 year to 18 years (average age - 8.19 ± 3.97 years), living in Moscow, who applied to the Center for Children's Allergology and Immunology of the Consultative and Outpatient Department GBUZ "DGKB No. 9 named after. G.N. Speransky Department of Health" in the period from 2017 to 2022 with complaints of allergic and non-allergic origin; Informed consent was obtained from the parents or legal representatives of the child to conduct the study. The clinical examination protocol was approved at a meeting of the ethics committee of the Federal State Autonomous Educational Institution of Higher Education Russian National Research Medical University named after. N.I. Pirogov of the Russian Ministry of Health.
All children were surveyed using a questionnaire developed by the authors as part of this study for the presence of GR for insect bites/stings. The questionnaire also makes it possible to establish an association between the development of symptoms and possible contact with insects, anamnestic prerequisites for the formation of IA, determine the severity of symptoms and clinical features of IA, the volume and effectiveness of therapy.
In the first part of the study, based on medical documentation data, 705 of 1587 children with confirmed atopic diagnoses were selected, including bronchial asthma (BA, ICD-10 code J45.9), year-round allergic rhinitis (cAR, ICD-10 code J30.4) , seasonal allergic rhinitis (sAR, ICD-10 code J30.1), atopic dermatitis (AD, ICD-10 code L20.9). Of these, the main group consisted of 247 children (average age - 7.17±3.69 years), who indicated during the questionnaire a history of GH symptoms of varying severity due to mosquito bites. Symptoms were observed mainly during the insect emergence season, which is typical for central Russia - from May to July. Control group 1 consisted of 426 children (average age - 8.12±3.95 years) who did not have GR for mosquito bites according to the questionnaire.
In the 2nd part of the study, the main group was compared with control group 2, which consisted of 14 children (average age - 5.7±3.56 years) without allergopathology and atopic predisposition, apparently healthy, with a history of GH symptoms due to mosquito bites.
Symptoms of pneumonia
The symptoms that precede pneumonia are similar to those of other respiratory diseases, so influenza may be diagnosed initially. However, symptoms vary greatly in severity.
The main and most common symptoms of pneumonia:
- fever and chills;
- chest pain;
- labored breathing;
- wheezing;
- cough;
- coughing up mucus;
- muscle pain;
- weakness;
- feeling overwhelmed and weak.
However, depending on the type of pneumonia, symptoms may vary. Thus, with atypical pneumonia, vomiting and diarrhea are also observed, and with bacterial pneumonia, a runny nose usually appears first. Any signs of pneumonia should not be underestimated and consult a doctor as soon as possible. Pneumonia in children has symptoms similar to those in adults, but is usually much more severe.
Anaphylaxis: some risk factors for its development
Anaphylaxis (AF) (the former term anaphylactic shock is no longer recommended) is a severe allergic reaction that develops quickly and can be fatal [1]. According to the World Health Organization, FA is a serious, life-threatening systemic hypersensitivity reaction. In fact, each of these definitions is inaccurate. It is clear that “life-threatening” reactions can be interpreted differently by both patients and physicians [2–5]. In particular, this was convincingly demonstrated in a recent study conducted in Germany, which revealed a significant underdiagnosis of FA among surveyed doctors [3].
Heterogeneous clinical symptoms of AF; misinterpretation of its clinical features; the lack of accessible and reliable tests confirming the diagnosis - all this undoubtedly makes it difficult to make a timely diagnosis of AF with a clear nosological classification in the daily clinical practice of a doctor of any specialty.
Recently, American experts, in a consensus document, proposed a definition of AF that generally satisfies epidemiological, research and clinical needs. According to the conclusion, AF is considered probable if the patient develops any of the following three criteria within a few minutes to several hours after exposure to an allergen (the presence of low blood pressure (BP) is not mandatory) (Table 1) [6, 7].
There are several important rules, the observance of which is tantamount to saving the life of a person with AF. A medical professional of any specialty is obliged to provide timely and correct assistance to such a patient. Moreover, such a patient must be able to give himself a life-saving injection of adrenaline, which greatly facilitates the use of an epinephrine auto-injector (unfortunately, still not available on the Russian pharmaceutical market) in the right situations. Every patient who has suffered a severe allergic reaction and AF (or suspected AF) must be referred to an allergist-immunologist. The responsibilities of an allergist-immunologist include: scrupulously detailing the medical history and coordinating allergological and other types of examination of such a patient; identify the cause that caused the development of AF; conduct training for the patient and provide him with a written plan for independent actions (they also teach abroad how to properly use an epinephrine auto-injector).
Classification
According to the modern international nomenclature of terms, allergic (caused by the participation of immunoglobulin E (IgE), formerly called “anaphylactic shock”) and non-allergic AF (the term “anaphylactoid shock” is considered obsolete) are distinguished (Fig.) [1, 2]. In non-IgE-mediated FA, immune responses may be initiated by IgG or other immune mechanisms (physical factors: eg, exposure to cold, heat, exercise; alcohol intake; medications (eg, opioids)). Idiopathic AF is a diagnosis of exclusion, which should be made only after a comprehensive in-depth examination of the patient (detail the medical history, exclude other causes of AF, including a previously unrecognized allergen; conduct a correct differential diagnosis, etc.). Currently, idiopathic AF is considered as a separate diagnosis, which, judging by the literature, opens up new opportunities for identifying previously unknown triggers of AF; requires studying pathophysiological mechanisms, as well as identifying patients with undiagnosed mastocytosis or clonal mast cell disease, etc.
Perhaps, apart from this division and practical validity, in general, nothing else significant has changed in the idea of FA since S. Kemp and R. Lockey wrote in their review in 2002: “there are no differences in the clinical picture and therapy, regardless of the pathophysiological mechanisms of development, between IgE- and non-IgE-mediated forms of AF” [8].
Many other terms are used to describe AF (generalized systemic reaction, systemic allergic reaction, severe hypersensitivity reaction), which undoubtedly also contributes to the underdiagnosis of AF and, especially, complicates its treatment (including the use of epinephrine) [9].
AF designations, according to ICD-10:
- T78.2 - Anaphylactic shock, unspecified.
- T78.0 - Anaphylactic shock caused by an abnormal reaction to food.
- T80.5 - Anaphylactic shock associated with serum administration.
- T88.6 - Anaphylactic shock caused by a pathological reaction to an adequately prescribed and correctly administered drug.
Prevalence
In general, true AF rates are underestimated because they are not recorded properly. There are several reasons, the main ones of which are: inaccurate coding according to ICD-10; inclusion in statistical data only of recognized cases of AF with a diagnosis established in a hospital; databases of regional hospitals were not included in the national Register, etc. [1–8]. According to the literature, the prevalence of AF is estimated at 10–20/10,000 cases per year [7]. The number of reported cases of FA in Alcorcon (Spain) was 103 episodes per 100,000 people per year (overall standardized incidence rate - 112); of these, most often (313 episodes) it occurred in the age group 0–4 years [4]. For comparison: there were extremely few requests for an appointment with an allergist-immunologist at one of the children's clinics in Moscow with diagnosed cases of FA in children, including other ages [5]. The general conclusion of most foreign studies is the same: over the past decades, the prevalence of FA has increased sharply in all age groups of the population. Thus, in Australia, the incidence of AF caused by food has increased in recent years by 350%, and for other reasons - by 230%. Drug-induced FA occurs in 1 in every 2,700 hospitalized patients.
Mortality
In the UK, for example, severe AF kills 1–3 people per million people annually (the main cause is nuts); in Australia, Turkey, Korea, and China, the main trigger for the fatal outcome of FA is drugs. Up to 20% of deaths due to FA are provoked by medications [9]. Risk factors for mortality from food-induced FA: age 10–35 years, exacerbation of bronchial asthma, peanut allergy, delayed administration of adrenaline. Risk factors for mortality in drug-induced FA: age 55–85 years, presence of respiratory and cardiovascular diseases; use of antibiotics or anesthetics. The most common cause of death from AF caused by hymenoptera insect bites is men aged 35–84 years (4–2 deaths per 1,000,000 population per year in the United States).
The main causes of death in AF: vascular insufficiency; asphyxia; vascular thrombosis; strokes; hemorrhages in the adrenal glands; hypotensive AF (from insect stings); obstruction of the upper/lower respiratory tract (with food-related AF); poorly controlled bronchial asthma [6–10].
Pathogenesis
FA, like allergies, develops as a result of immune reactions mediated by IgE, which, through high-affinity FcεRI receptors, participates in the release of many inflammatory mediators from activated mast cells and basophils (histamine, heparin, tryptase, chymase, carboxypeptidase A3, tumor necrosis factor alpha ( TNFa); de novo synthesized - platelet activating factor (PAF), prostaglandin D2 (PGD2), leukotriene C4, interleukins (IL-5, 6, 8, 13), chemokines (MIP-1, MIP-1b, MCP-1) etc.) [1, 6, 7].
Mast cells play a key role not only in the development of FA. They are widely represented in the respiratory tract, including the alveoli of the human lungs, in the gastrointestinal tract, and skin. It is believed that recurrent episodes of FA occur in individuals with higher mast cell counts; or the reason is due to different pathways of their activation, which may explain the predisposition of some people to recurrence of AF. Increased levels of mast cells and IgE in the bronchi are characteristic signs of allergic asthma. High levels of IgE can lead to increased expression of FcεRI receptors on mast cells. Theoretically, the presence of such receptors on mast cells in the alveolar parenchyma increases the risk of AF in patients sensitized to systemic allergens in bronchial asthma.
Activation of histamine through H1-H4 receptors leads to coronary vasoconstriction and heart failure (H1 receptors), systemic vasodilation and tachycardia (H2 receptors), inhibition of norepinephrine release (H3 receptors), chemotaxis and release of inflammatory mediators (H4 receptors). Heparin and, possibly, tryptase promote the activation of bradykinin, fibrinolysis processes and the complementary system. Platelet-activating factor reduces coronary blood flow and myocardial contractility, enhances the activation of neutrophils and eosinophils, causes local and systemic platelet aggregation, as well as peripheral vasodilation and severe hypotension, possibly through the induction of NO. Due to physiological changes caused by AF, compensatory mechanisms are activated, including the renin-angiotensin-aldosterone system, increased secretion of neuroepinephrine from local sympathetic nerve endings, which can lead to cardiac arrhythmia, etc. Their negative effect is enhanced by the action of tryptase, which released from degranulated mast cells [10].
Yet, traditionally, the immunopathological mechanisms of FA are focused on IgE-dependent and independent release of mediators from mast cells and basophils. However, recently, evidence has accumulated that supports the importance of alternative pathways for the development of AF. Indeed, there are many cases when a person who has suffered from FA does not have antigen-specific IgE or there are no signs of mast cell activation (increased serum levels of tryptase, histamine). In other words, the classical pathway, which involves IgE, mast cells and histamine, cannot explain every cause of FA. This was shown in experiments on mice deficient in mast cells, IgE, or their receptors FcεRI [11]. Thus, the serum level of platelet-activating factor correlates well with the severity of AF in humans [12].
Idiopathic AF is diagnosed in cases where, based on the medical history, results of skin tests and in vitro tests (determination of specific IgE antibodies in the blood serum, if possible, in combination with cellular reactions), it is not possible to detect the cause of AF.
Risk factors
Assessing risk factors is extremely important, since they are also involved in the development of FA and, perhaps, play a dominant role in confirming the diagnosis and choosing therapy. However, some people develop allergic reactions in the absence of any obvious risk factors. However, there are a number of clinical situations in which the risk of developing FA increases (Table 2) [6–10, 13].
Individuals with atopy have an increased risk of developing serious allergic reactions to medications. Age (drug allergies are more common in young and elderly people), genetic polymorphism of the human leukocyte antigen (HLA, the major histocompatibility complex gene), as well as concomitant viral infections (human immunodeficiency virus (HIV), Epstein-Barr virus (EBV), viruses herpes) are also associated with an increased risk of developing immunological reactions to drugs. Susceptibility to drug allergies also depends on genetic polymorphisms in drug metabolism. In addition, the method of drug administration is relevant (the intravenous route is associated with a more severe reaction and the development of AF).
Experience shows that patients with previous unexplained reactions during anesthesia are also at risk for developing allergic reactions. In addition, multiple surgeries, procedures, occupational exposure to antibiotics, latex, etc. are associated with an increased incidence of FA.
Etiology
Foods, medications, and insect bites are the three most common triggers for AF. In children, the most common cause of FA is food, while in adults it is insect poison and drugs (Table 3) [4, 7–9].
Anaphylaxis to food
All foods have the potential to cause FA, including those that have not previously been observed to cause such reactions (for example, fresh red meat containing carbohydrate determinants, which is especially common in individuals with a history of tick bites). Additionally, food triggers may be hidden in substitutes; cross-reactive foods; in food additives (spices, dyes - carmine/cochineal, monosubstituted glutamate, sulfites, papain). Reactions can also be caused by parasites contaminating food (for example, the nematode Anisakis simplex) and dust mites. In particular, cases of the so-called food tick-borne anaphylaxis (Oral Mite Anaphylaxis; OMA; Pancake Syndrome) are described - an allergic reaction to poisoning by food contaminated by ticks. Living in old flour, various dry medicinal plants and in warehouses, the tick Thyreophagus entomophagus (common in Europe, found in the Russian Federation) can cause occupational respiratory diseases in farmers (pulmonary acariasis), as well as food-borne tick anaphylaxis. A patient sensitized to house dust mites who has eaten products made from flour infected with T. entomophagus develops urticaria, itching, cough, wheezing, and AF. The causative agent may also be ticks Blomia freemani, Dermatophagoides pteronyssinus, Dermatophagoides farinae and Blomia tropicalis. Such cases are more often diagnosed in tropical and subtropical climates.
It was food products (nuts, especially cashews, peanuts, milk, eggs) that were the main cause of FA (92% of cases) registered in Stockholm during the year in children [14]. It was more often observed during the flowering period, as well as in children suffering from bronchial asthma. In a retrospective study of 220 patients aged 50–65 years, the incidence of food-related AF was also the highest at 42% [15].
Anaphylaxis to latex
There are three risk factors for the development of AF and allergic reactions to latex: 1) medical workers; 2) children with Spina bifida and urogenital malformations; 3) professional latex exposure. In such risk groups, patients, along with taking into account medical history (only a survey does not provide complete information!), to diagnose latex allergy, use skin tests, patch tests, a test with latex gloves, as well as the determination of specific IgE antibodies to latex. Unfortunately, there are no standard tests for diagnosing allergies to natural latex [2]. For such patients, latex-free items (catheters, gloves, etc.) are used during dental procedures and surgical interventions.
Anaphylaxis to medications
Approximately 10% of adverse drug reactions are unexpected drug hypersensitivity reactions. There are frequent cases of both underdiagnosis and overdiagnosis [9].
Drugs can cause FA through IgE-dependent, IgE-independent immunological mechanisms or direct stimulation of mast cells. The most common cause of drug hypersensitivity reactions are antibiotics (primarily beta-lactams); vaccines and hormones (eg, progesterone, insulin, ACTH); protein preparations (immunoglobulins), as well as vitamin B, local anesthetics, non-steroidal anti-inflammatory drugs, allergens used for immunotherapy.
There have been reports of FA occurring with the use of monoclonal antibodies (setuximab, infliximab, omalizumab). In particular, AF due to omalizumab develops in 0.09% of cases, in 61% 2 hours after the 3rd injection and in 14% 30 minutes after the 4th–5th injection [16]. There are cases where AF occurred in patients with severe bronchial asthma 1 year after the start of omalizumab therapy.
During anesthesia, the development of AF depends on a very wide range of factors, including latex; the use of many drugs, as well as non-anesthetic agents (for example, disinfectants, antiseptics). According to the literature, AF that developed during general anesthesia is most often associated with neuromuscular blockers, latex and antibiotics [2].
Vaccines to prevent infectious diseases rarely cause FA (rather, it may be proteins such as gelatin, dextran, or ovalbumin in eggs). Recently, cases of AF were described 1 year after the use of DPT in children with an allergy to cow's milk, which scientists associated with the casein contained in this vaccine (it is known that the level of specific IgE antibodies to cow's milk proteins does not necessarily correlate with the severity of allergic reactions) [17].
Anaphylaxis to allergen-specific immunotherapy (ASIT)
First of all, ASIT is carried out only by specially trained allergist-immunologist and a nurse, which greatly reduces the risk of developing FA (other allergic reactions) to immunotherapy.
When ASIT is performed correctly, the incidence of severe and fatal reactions is very low (1 case in approximately 2,500,000 injections) [16]. The risk is increased in patients with poorly controlled asthma or taking beta-blockers.
If FA appears during ASIT, the allergist-immunologist must identify factors related directly to the immunotherapy itself, on the one hand, and the patient’s health status, on the other (Table 4) [18].
Anaphylaxis to seminal fluid
FA after sexual intercourse is considered to be the result of IgE-mediated sensitization to seminal plasma proteins of different molecular weights (> 90% of prostate-specific antigens have a molecular weight of 12–75 kDa). Most of these patients had a history of severe sensitization to dogs [2].
The disease is diagnosed based on prick tests with fresh human seminal plasma or its fractions. However, in such patients other causes of allergies should be excluded (latex, food allergy, passive transfer of the allergen through seminal plasma).
Anaphylaxis on exercise
Strong physical activity can provoke or aggravate syndromic manifestations of allergies and even FA [2, 9]. Usually, after extreme stress (playing football, tennis, aerobics, dancing), as well as overheating, some patients may develop a urticarial rash, itchy skin and progression of symptoms to the development of angioedema, wheezing, and collapse. Sometimes these episodes are associated with food intake (a specific food to which the patient is sensitized); medications (for example, aspirin, other non-steroidal anti-inflammatory drugs) or coincide with a period of high pollen concentrations in the air [2, 19].
Most often, taking an allergenic product 2–4 hours (less often 12 hours) before physical activity leads to the appearance of skin itching or other symptoms listed above in such patients [2].
In such cases, you should immediately stop physical activity. Preventive medication is not effective; some patients may benefit from daily antihistamines [2]. The prognosis is good, but deaths have been described. Severe attacks pass over time, apparently due to the patient avoiding physical activity or changing living conditions.
Rarer causes of AF are physical factors (cold, heat, water). In patients suffering from cold urticaria, AF may develop due to general hypothermia (for example, swimming in cold water).
Occupational allergens, and less commonly inhalation of allergens such as animal dander or grass pollen, can also cause FA [2].
Insect bite
In some people, an allergy to hymenoptera venom can cause FA, which can be fatal. The occurrence of abdominal symptoms (abdominal pain and vomiting) soon after a hymenoptera insect bite is a predictor of the development of FA. If the diagnosis of insect allergy is confirmed, ASIT is indicated for a patient who has suffered from AF due to a hymenoptera sting (according to foreign studies, it is effective in 98% of cases). However, some patients have a convincing history indicating AF, which arose in response to an insect bite, but negative results of an allergological examination (since skin tests with extracts of insect venom are not available in the Russian Federation, the levels of specific IgE antibodies are determined in such patients). This situation requires exclusion in a patient with mastocytosis: recently, scientists have drawn attention to a sharp increase in the prevalence of AF in such patients.
Idiopathic anaphylaxis
Sometimes AF can develop for no apparent reason. Such patients should be carefully examined (detailed analysis of the medical history to exclude all suspected causes of FA in combination with specific laboratory tests, for example, to exclude indolent systemic mastocytosis). Other clinical situations: unexplained AF or AF accompanied by severe cardiovascular symptoms (hypotension and syncope in the absence of urticaria), in which clonal mast cell disorders should also be suspected [20]. In patients with undiagnosed mastocytosis, a history of unusual sensations following exposure to heat (hot showers) or alcohol (two of the strongest mast cell activators) or unexplained fractures may be helpful additions. Idiopathic recurrent AF may accompany sluggish (indolent) mastocytosis, in which there may be no skin manifestations. Thus, 22–49% of adult patients suffering from systemic mastocytosis experience episodes of severe AF.
Sometimes a doctor suspects a vasovagal reaction in a patient with AF.
Vasovagal collapse (neuropsychological reaction) is fainting that develops in a patient after injections or other painful manipulations and is manifested by a weak pulse, pallor of the skin, severe sweating, and nausea. Blood pressure is most often normal. Skin itching, urticaria, angioedema, tachycardia, difficulty breathing and other signs characteristic of AF are absent.
Thus, summarizing the literature data on the role of risk factors for the development of AF, we can highlight: 1) age-related factors; 2) with concomitant diseases (in particular, the patient’s atopic status is a risk factor for the development of AF to triggers such as food, physical activity, latex, but not hymenoptera venom); 3) simultaneous use of medications (especially beta-blockers, ACE inhibitors, sedatives, antidepressants) and alcohol; 4) the presence of co-factors (physical activity: acute infection, for example, ARVI; premenstrual period; emotional stress; travel), which increase the manifestations of AF.
In other words, quite a lot of risk factors and co-factors contribute to the development or worsening of the course of AF, of which the doctor should be aware as fully as possible, since all these factors also play a leading role in the diagnosis and treatment of this severe life-threatening reaction.
Literature
- Simons E., Ardusso L., Bilo V. et al. World Allergy Organization anaphylaxis guidelines: Summary // J. Allergy Clin. Immunol. 2011; 127:587–593.
- Lieberman P., Nicklas R., Oppenheimer J. et al. The diagnosis and management of anaphylaxis practice parameter // Ibid. 2010; 126:477–480.
- Mehl A., Wahn U., Niggemann B. Anaphylactic reactions in children - a questionnaire-based survey in Germany // Allergy. 2005; 60: 1440–1445.
- Alonso T., Moro M., Garcia M. et al. Incidence of anaphylaxis in the city of Alcorcon (Spain): a population-based study // Clin. Exp. Allergy. 2012; 42:578–589.
- Macharadze D. Sh. Pilot screening of allergic diseases during clinical examination of Moscow schoolchildren // Russian Journal of Allergology. 2006, No. 4, p. 28–32.
- Campbell R., Hagan J., Manivannan V. et al. Evaluation of National Institute of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network criteria for the diagnosis of anaphylaxis in emergency department patients // J. Allergy Clin. Immunol. Published online 03 November 2011.
- Simons E. Anaphylaxis//Ibid. 2010; 125:S161–181.
- Kemp S., Lockey R. Anaphylaxis: a review of causes and mechanisms // Ibid. 2002; 110:341–348.
- WAO White Paper on Allergy 2011–2012: Summary. Ed. R. I. Sepiashvili, T. A. Slavyanskaya. M.: Medicine-Health, 2011, 12 p.
- Khan B., Kemp S. Pathophysiology of anaphylaxis // Curr. Opin. Allergy Clin. Immunol. 2011; 11: 319–325.
- Finkelman F., Rothenberg M., Brandt E. et al. Molecular mechanisms of anaphylaxis: lessons from studies with murine models // J. Allergy Clin. Immunol. 2005; 115:449–457.
- Karasuyama H., Obata K., Wada T. et al. Newly appreciated roles for basophils in allergy and protective immunity // Allergy. 2011; 66:1133–1141.
- Muraro A., Roberts G., Clark A. et al. The management of anaphylaxis in childhood: position paper of the European Academy of Allergology and Clinical Immunology // Ibid. 2007; 62:857–871.
- Vetander M., Helander D., Flodstrom C. et al. Anaphylaxis and reactions to foods in children — a population-based case study of emergency department visits // Clin. Exp. Allergy. 2012; 42:568–577.
- Campbell R., Hagan J., Li J. et al. Anaphylaxis in emergency department patients 50 or 65 years or older // Ann. Allergy Asthma Immunol. 2011; 106:401–406.
- Cox L., Nelson H., Lockey R. et al. Allergen immunotherapy: a practice parameter third update // J. Allergy Clin. Immunol. 2011; 127(Suppl. 1): 1–55.
- Kattan J., Konstantinou G., Cox A. et al. Anaphylaxis to diphtheria, tetanus, and pertussis vaccines among children with cow's milk allergy // Ibid. 2011; 128:215–218.
- Liss G., Murphy-Berendts K., Epstein T., Bernstein D. Factors associated with severe versus mild immunotherapy-related systemic reactions: a case-referent study // Ibid. 2011; 127:298–300.
- Macharadze D. Sh. Anaphylaxis caused by physical activity // Allergology and immunology. 2002, vol. 2; With. 192–94.
- Akim S. Anaphylaxis and Mast Cell Disease: What Is the Risk? //Curr. Allergy & Asthma Reports. 2010; 10:34–38.
D. Sh. Macharadze, Doctor of Medical Sciences, Professor
RUDN University , Moscow
Contact information about the author for correspondence
Diagnosis of pneumonia
Pneumonia is not easy to diagnose. Lung noises may not be heard even by the most qualified doctors. In this case, it is worth taking a chest x-ray to assess the degree of inflammation. The doctor also diagnoses the disease after conducting a blood test (complete blood count, PCT, ESR and CRP).
Respiratory cultures for microbiological tests and blood cultures are also performed to diagnose pneumonia. Inpatients are also prescribed computed tomography and bronchoscopy.
Research methods
The study was carried out on the basis of a general clinical (complete blood count with leukocyte formula) and specific allergological examination of patients (questioning; collection of allergic, food, insect history; determination of the level of total immunoglobulin IgE in the blood serum of patients using the enzyme-linked immunosorbent assay using the diagnostic kit "Total IgE -ELISA" (Labmedtest, Russia). Determination of the levels of specific IgE in blood serum was carried out using the immunofluorescence reaction (IFL) method on the three-dimensional porous solid phase ImmunoCAP (Pharmacia Diagnostics AB, Switzerland). Determination of the levels of specific IgE was carried out to allergens of pyrolyphoid mites ( Dermatophagoides pteronyssinus
,
Dermatophagoides farinae
), insects (cockroach, mosquito, wasp venom, honey bee venom), seafood (shrimp), fish (cod, salmon), dog hair, cat hair, tree pollen mixture (birch, alder, hazel), pollen mixture cereal grasses (timothy, fescue, ryegrass, rye), a mixture of weed pollen (wormwood, ragweed, quinoa). The interpretation of the obtained IPF results was carried out according to the generally accepted system of IgE concentrations: ≤0.35 kU/l - clinically insignificant level (class 0); 0.36–0.69 kU/l - 1st level; 0.7–3.49 kU/l - level 2; 3.5–17.49 kU/l—level 3; 17.5–49.9 kU/l—level 4; 50–99.9 kU/l - 5th level, more than 100 kU/l - 6th level.
Statistical processing
The obtained results were carried out using the Microsoft Excel-5 application package (Microsoft, USA), the SPSS statistical package version 6.0, and the Biostatistica program (IBM Company, USA). The results of the study were processed and compared statistically using Student's t-test. Differences were considered significant at a p value of less than 0.05. To assess the significance of differences between laboratory parameters in the study groups, the nonparametric Wilcoxon test was used.
Treatment of pneumonia
Pneumonia, diagnosed at an early stage, is easily treatable. Doctors usually prescribe drugs that help cough up secretions, antipyretics, and strong antibiotics.
A person with typical pneumonia recovers in 7–10 days. Bacterial pneumonia lasts longer - up to 21 days. In addition to taking medications, it is also important to drink plenty of water. With pneumonia (when the patient does not have a fever), there is no need to lie in bed. Doctors even recommend doing sports, especially outdoors. Medicines are prescribed to improve ventilation and remove residual secretions.
In some cases, a doctor may refer a person with pneumonia to the hospital. In severe cases of the disease, the child requires hospitalization. The hospital prescribes intravenous antibiotic therapy. Fortunately, these are not common cases.
Etiology of reactions to insect bites
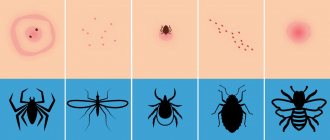
Allergic and toxic reactions are caused directly by bites and other effects of various insects. Hymenoptera pierce the skin with a sting and release poison into the resulting wound, to which the body can react accordingly. So, bites:
- mosquitoes are accompanied by itching and an allergic reaction with swelling, rash, and sometimes fever;
- fleas cause dematoses, increased body temperature, and a rash similar to hives;
- bedbugs provoke various reactions, ranging from ordinary itching to anaphylactic shock;
- mosquitoes cause the formation of itchy papules, burning skin, nausea, vomiting, secondary rashes;
- Horseflies cause local swelling, redness, the appearance of tumors, swelling of the lymph nodes;
- midges lead to the formation of papules, swelling, development of hyperemia and tachycardia.