Classification. Malarial plasmodium: type Apicomplexa , class (Sporozoa) Sporozoa . They belong to the order Cococidia (Eucoccidiida) , suborder Blood Sporidae (Haemosporina) and genus Plasmodium .
This type includes a great many species, but only four species are parasitic and are the causative agents of malaria. It is a single-celled protozoan “just one tiny cell” that acts as an independent parasite.
During their existence, parasites go through several stages. The malarial plasmodium first divides, grows, then changes, just like everything can reproduce both sexually and asexually.
Life cycle
The cycle of life is a very complex development. In humans it can be the causative agent of the well-known disease malaria.
A person can become infected only if he is bitten by a female malaria mosquito, whose secretion contains the pathogen at a certain stage (sporozoite). Humans are the intermediate host of Plasmodium falciparum. The main host of Plasmodium falciparum is the female mosquito.
Let's consider this cycle. First, a person must be bitten by an infected female, which will carry (the malaria virus itself) sporozoites of the malaria mosquito, which in turn enter the bloodstream, attach to red blood cells (erythrocytes) and are found in the liver. Where does “pre-erythrocytic schizogony” occur? It can be compared with the initial period of the disease.
Tissue schizonts begin to develop from sporozoites located in liver cells. Then they enlarge and division occurs by schizogony (multiple asexual reproduction of protozoa). After this, the liver begins to decompose, namely its cells, and parasites in the merozoite phase penetrate into the blood.
Attached to red blood cells, they degrade hemoglobin in the blood and also reproduce asexually. Schizonts grow due to nutrition with hemoglobin, passing into the stage of amoeboid schizonts; but even after this they do not stop destroying hemoglobin (feeding on it); they stretch out, take the shape of a circle, their nuclei multiply repeatedly.
This phase is called morula, and blood merozoites are cells dividing erythrocyte schizogony. If the protective membrane of the red blood cell disintegrates under the influence of merozoites, they will be released into the blood and then into the plasma (merulation). When this happens, the infected person has an outbreak of malaria. This is expressed in excessive agitation (fever); a person feels cold and shudders.
Merozoites again enter the red blood cells and the cycle of erythrocytic schizogony is repeated again and again. After several cycles, preparations for sexual reproduction occur.
Some group of merozoites turns into germ cells (so-called gametocytes). Female gametocytes are larger in size than male ones. Only their subsequent formation is likely only in the body of the malaria mosquito.
If this sick person is bitten by a mosquito, it will be in his stomach. Merozoites that divide asexually die or are digested in the digestive tract, and gametocytes enter the gamete phase (mature form). Male and female gametes unite. As a result of their union, a zygote appears, consisting of one cell.
After this, the zygote passes into the intestine of the mosquito, increasing in size, becoming a very large oocyst. After some certain time, it crumbles, and a fairly decent number of sporozoites emerge (this development is called sporogony). The sporozoites then move to the brain and are collected in the salivary glands. The sporangia are now transferred to the next host (human).
General characteristics of the microorganism
The malarial plasmodium belongs to the phylum Sporozoan and represents a subkingdom of protozoa leading a parasitic lifestyle. This single-celled microorganism causes a fatal disease. Plasmodium, unlike other multicellular microorganisms, consists of a single cell that is capable of breathing, moving, feeding and reproducing.
The toxins secreted by parasites lead to high temperatures and occasional bouts of fever.
The time interval after which the attack will resume depends on the type. This period coincides with the destruction of red blood cells, which carry oxygen throughout the body. Signs of anemia appear.
Some types of malarial plasmodia can live in the environment:
- three-day, causing malaria of the plasmodium vivax type (develops in the human body from one to three weeks, sometimes the first signs can appear after six months);
- the provocateurs of four-day malaria are malariae (the incubation period is one month);
- the development of malaria occurs as a result of the bite of mosquitoes of the genus falciparum, living in tropical countries (the incubation period lasts from 10-20 days);
- another three-day species is ovale (the incubation period lasts about two weeks);
- a two-day-old species of knowlesi leads to severe consequences.
The parasite enters in several ways. The most basic is the bite of an Anopheles mosquito. But there are other ways of infection, for example, blood transfusion. The infection can reach the fetus during pregnancy or during childbirth from a sick mother.
The intermediate host of Plasmodium falciparum is humans. During a bite, saliva is released, which contains sporozoites. They have a curved, elongated body shape, size about 15 microns. Plasmodium malaria has a parasitic effect in relation to humans.
Where does Plasmodium falciparum live? The parasite requires warmth to develop. Therefore, the risk of contracting the disease increases in countries with warm climates. The most dangerous countries are considered to be Brazil, Vietnam, Europe, and Colombia. There may be infection with malarial plasmodium on the coast of the Red and Mediterranean Seas. Ukraine, Kazakhstan, Georgia, and Azerbaijan are no exception. Found in Russia and Belarus.
Phases of malaria
In general, there are four phases of malaria in the world. A certain form has its own characteristics. The only common symptoms are fever, anemia and enlargement of internal organs (such as the liver and spleen).
- " Three-day malaria ". A week before the onset of attacks, chills, headaches, a feeling of weakness and despair begin, and nausea appears. Afterwards the attacks themselves begin, they have an alternating character (chills, fever, sweating). The liver and spleen enlarge, and anemia begins. The disease lasts two or three years.
- " Quadrennial malaria ". It occurs in a mild form. First, a fever begins, the internal organs become slightly enlarged, and anemia does not always develop. There is an increase in pressure, swelling, and a large amount of protein is removed along with the urine. It appears more often in children. It lasts for a very long time, from three to fifty years.
- " Tropical malaria ". Immediately pronounced malaise, weakness, headaches, joint pain, a sharp decrease in appetite, nausea, mild chills. The fever is constant and kidney function is impaired. These symptoms complicate the detection of malaria, which leads to severe manifestations (coma, renal failure). The duration of the disease is up to one year.
- " Malaria ovale " Symptoms are similar to "three-day malaria". Fever begins much earlier, the duration of the disease is three, four years.
There is the concept of “malarial coma” - this is a corresponding deviation in tropical malaria, characterized by a very stormy, progressive and complex prognosis. There are three phases of coma: “somnolence”, “stupor” and “deep coma”, in which death is close to 100%.
Routes of transmission
Malarial plasmodia most often enter the human body through transmission through the bites of female mosquitoes that carry the parasites. But there are several other ways of infection with these protozoa:
- Transplacental. Possible in the complete absence of immunity to malaria in the expectant mother. Infection occurs during childbirth or in the event of placental abruption in a pregnant woman who is a carrier of Plasmodium.
- Transfusion method of infection. Infection occurs in this way in people who have received a blood transfusion from a malaria patient. When storing biomaterials in the refrigerator, plasmodia do not die within 2 weeks.
- Parenteral. This way you can become infected through blood-contaminated medical needles. People who inject drugs are often infected through transfusion.
Causes of malaria
In areas with high endemic rates of malaria, children from 6 months to 5 years were recognized as the main sources of parasites. They often get sick in an atypical form, which contributes to late diagnosis and the development of an infectious focus. As a result, the disease spreads several times faster.
Symptoms of malaria
This is an acute convulsive disease. In the intermediate host (human), who has a weak immune system, signs of the disease are visible within one or two weeks after the actual carrier (female malaria mosquito) transmits the disease.
The first sign is a feverish state, headache, chills, and possible vomiting. Symptoms may not be pronounced, which slows down the detection of malaria in the initial stages.
If the disease is prolonged, the intermediate host may die. Complications that can worsen a person’s condition: the number of red blood cells decreases, namely hemoglobin (anemia or anemia), the liver, lungs are affected, heart failure may occur, brain activity is damaged (resulting in convulsions, loss of consciousness, paralysis or even coma), loss consciousness, all this leads to death.
Origin of the species and description
Photo: Malaria mosquito
The malaria mosquito is a dipterous insect, an obligate bloodsucker from the suborder Long-whiskered, which is a carrier of malarial plasmodia, which are considered the most dangerous parasites for humans. The Latin name for this species of arthropod is Anopheles, which translates as harmful, useless. There are 400 varieties of Anopheles, many of them are capable of transmitting malaria, as well as being the main host for a number of other dangerous parasites.
Video: Malaria mosquito
Several fossil varieties are known from Oligocene and Dominican amber deposits. Some historians believe that malaria was the main cause of the fall of the Western Roman Empire in the fifth century. At that time, epidemics broke out in the coastal regions of Italy. The draining of numerous swamps and the construction of new roads resulted in almost constant brutal malaria for the inhabitants of Rome. Hippocrates also described the symptoms of this disease and associated the onset of malaria epidemics with natural conditions.
Interesting fact: Malaria mosquitoes look at the world through the prism of infrared rays, so they are able to find warm-blooded animals and people even in pitch darkness. In search of an object to receive a portion of food - blood, these arthropods can fly over distances of up to 60 kilometers.
Diagnostics
If a person develops the first symptoms and is at risk.
The first thing he should do is take a blood test and conduct a biochemical analysis, which will reveal anemia (low hemoglobin and red blood cells), low platelet levels and an excessive white blood cell count.
The second test is to determine malarial plasmodia in the blood (detailed examination of a drop of blood). If detected, specific therapy is prescribed.
Historical aspects
The historical focus of this disease is Africa. From this continent, malaria spread throughout the world. At the beginning of the 20th century, the number of cases was about 700 million per year. One out of 100 infected people died. The level of medicine of the 21st century has reduced morbidity to 350-500 million cases per year and reduced mortality to 1-3 million people per year.
Malaria was first described as a separate disease in 1696, at the same time the official medicine of that time proposed treating the symptoms of the pathology with cinchona bark, which had been used by folk medicine for a long time. The effect of this medicine could not be explained, because in a healthy person, quinine, when taken, caused complaints similar to fever. In this case, the principle of treating like with like, which was preached by Samuel Hahnemann, the founder of homeopathy, was applied in the 18th century.
The name of the disease that is familiar to us has been known since 1717, when the Italian physician Lancini established the cause of the development of the disease, coming from the “rotten” air of swamps (mal`aria). At the same time, suspicion arose that mosquitoes were responsible for transmitting the disease. The 19th century brought many discoveries in establishing the causes of malaria, describing the development cycle and classifying the disease. Microbiological studies made it possible to find and describe the infectious agent, which was named malarial plasmodium. In 1897 I.I. Mechnikov introduced the pathogen into the classification of microorganisms as Plasmodium falciparum (class of sporozoans, type of protozoa).
In the 20th century, effective drugs were developed to treat malaria.
Since 1942 P.G. Müller proposed the use of the powerful insecticide DDT to treat areas of disease outbreaks. In the middle of the 20th century, thanks to the implementation of the global malaria elimination program, it was possible to limit the incidence to 150 million per year. In recent decades, an adapted infection has launched a new attack on humanity.
Treatment
Currently, there are a large number of drugs that can alleviate and even completely cure patients with malaria; the main thing is to diagnose it at the initial stage. Medicines are used in accordance with the type of parasite and the area where it is located.
Medicines most often need to be taken orally (tablets, capsules). In advanced cases, intravenously. Malaria is one of those diseases that can make itself known (come back) at any time.
Dormant merozoites may persist in liver cells. If symptoms reappear, you should immediately contact a specialist. It is strictly prohibited to donate blood for more than three years.
Classification
As noted above, there are separate types of parasitic pathogens of the disease. Each form of infection can provoke the development of pathologies with its own specific characteristics. To avoid confusion when diagnosing and drawing up a treatment program, the following classification of malarial plasmodium has been developed:
- Malariae-malaria is an infectious pathogen characterized by an incubation period of 4 days.
- Plasmodium vivax is a three-day variant of malaria.
- Plasmodium ovale is another form of the pathogen, when infected, the first symptoms appear within 3 days.
- Falciparum is a tropical type of infection.
- Plasmodium knowlesi is the most dangerous class of malaria pathogen, since in this case the phase of active reproduction of the parasite in the host’s blood begins after 24 hours.
Prevention
Unfortunately, there are no vaccines against malaria; they are still in the process of being created. The main task of a person is to protect himself from mosquito bites and take antimalarial medications under the supervision of a specialist.
If you find yourself in a risk zone (hot countries), you should follow some rules:
- The main thing is to protect yourself from mosquitoes (namely bites), you should wear thick clothing, especially at night.
- The use of certain detergents should be used as often as possible, since they have the property of weathering.
- Before traveling to hot countries, you need to consult a specialist on the use of antimalarial drugs.
be careful
According to statistics, more than 1 billion people are infected with parasites. You may not even realize that you have become a victim of parasites.
In men, parasites cause: prostatitis, impotence, adenoma, cystitis, sand, kidney and bladder stones.
In women: pain and inflammation of the ovaries. Fibroma, myoma, fibrocystic mastopathy, inflammation of the adrenal glands, bladder and kidneys develop. As well as heart disease and cancer.
We would like to warn you right away that you do not need to run to the pharmacy and buy expensive medications, which, according to pharmacists, will eradicate all parasites. Most medications are extremely ineffective, and they also cause great harm to the body.
There is also immunity to malaria
- " Innate immunity ". Intermediate carriers with a genetic indicator show some resistance to parasites.
- " Acquired active immunity ". It appears only when a person has had this disease. The level of immunoglobulins increases.
- " Acquired passive immunity" . It appears when ready-made antibodies are introduced into the body.
Sources
- Guide to Medical Entomology / ed. V. P. Derbeneva-Ukhova. – M.: Medicine, 1974. – 359 p.
- Yatusevich, A.I. Little-studied infectious and parasitic diseases of domestic animals: textbook / A.I. Yatusevich, N.N. Androsik. – Mn.: Urajai, 2001. – 331 p.
- Parasitology and invasive diseases of agricultural animals / K.I. Abuladze [and others]. – M.: Agropromizdat, 1990. – 464 p.
- Workshop on parasitology and invasive animal diseases: textbook / A.I. Yatusevich [etc.]. – Mn.: Urajai, 1999. – 279 p.
- Kapustin, V. F. Atlas of blood parasites of animals and ixodid ticks / V. F. Kapustin. – M.: State. ed. agricultural literature, 1955. – 216 p.
- Diagnosis, therapy and prevention of parasitic diseases of horses. UMP for students majoring in veterinary medicine and FPC students. /A.I. Yatusevich, S.I. Stasyukevich, M.P. Sinyakov, V.V. Petrukovich./ Vitebsk, VGAVM, 2011, 60 pp.
- Bulanova-Zakhvatkina, E. M. Armored oribatid mites / E. M. Bulanova-Zakhvatkina. – M.: Higher School, 1967. – 254 p.
- Yatusevich, A.I. Eimeriosis of chickens and its parasitocenological aspects / A.I. Yatusevich, A.V. Sandul, V.N. Gisco. – Vitebsk: VGAVM, 2009. – 249 p.
- Parasitology and invasive diseases of farm animals / K. I. Abuladze, N. V. Demidov, A. A. Napoklonov, etc.; edited by K. I. Abuladze. – 3rd ed. – M.: Agropromizdat, 1990. – 464 p.
- Balashov, Yu. S. Blood-sucking ticks (Ixodoidea) - carriers of human and animal diseases / Yu. S. Balashov. – L.: Nauka, 1967. – 320 p.
- Determinant of helminths of hunting mammals in Belarus: monograph / A.I. Yatusevich [and others]. – Vitebsk: VGAVM, 2010. – 228 p.
- Veterinary and sanitary measures for the prevention and elimination of parasitic diseases of animals: guidelines / I.N. Dubina [and others]. – Vitebsk: VGAVM, 2008. – 51 p.
- Dubina, I.N. Veterinary and sanitary rules for the prevention and elimination of animal cestodiasis: approved. GUV MASHIP RB / I.N. Dubina, A.I. Yatusevich. – Vitebsk: VGAVM, 2007. – 10 p.
- Yatusevich, A.I., Parasitic diseases of birds / A.I. Yatusevich, B.Ya. Birman, T.G. Nikulin. – Mn.: Publishing house Polibig, 2001.
- Olenev, N. O. Scabies mites / N. O. Olenev. – L.: Ed. Academician Sciences of the USSR, 1932. – 64 p.
- Kuznetsov, M.I. Anoplocephalatosis of ruminants / M.I. Kuznetsov. – M.: Kolos, 1972.
- Stepanova, N.I. Protozoal diseases of animals / N.I. Stepanova. – M.-L.: Kolos, 1982.
- Adaptation processes and parasitosis of animals: monograph / A.I. Yatusevich [and others]. – Vitebsk: OU VGAVM, 2006. – 404 p.
- Yatusevich A.I., Poorly studied infectious and invasive diseases of domestic animals / A.I. Yatusevich, N.N. Androsik. – Mn.: Urajai, 2001. – 332 p.
- Dubinina, M. N. Parasitological studies of birds / M. N. Dubinina. – L.: Nauka, 1971. – 139 p.
- Savchenko, S.V. Prevention and treatment of balantidioesophagostomotic infestation in pigs / S.V. Savchenko, V.F. Savchenko. – Vitebsk: VGAVM, 2010. – 194 p.
- Theoretical and practical principles of the use of medicinal plants for parasitic diseases of animals / A.I. Yatusevich [and others]. – Vitebsk: VGAVM, 2008. – 75 p.
- Dubinin, V. B. Scabies mites. Biology, harm in agriculture, measures to prevent and combat them / V. B. Dubinin. -M.: Soviet Science, 1954. – 173 p.
- Yatusevich, A.I. Arachnoenthomoses of domestic ruminants and single-hoofed animals: monograph / A.I. Yatusevich [and others]. – Vitebsk: VGAVM, 2006. – 213 p.
- Subbotin, A.M. Sparganosis of wild boar: differential diagnosis and improvement of measures to combat it in the conditions of the Republic of Belarus: method. instructions / A.M. Subbotin, N.F. Karasev, V.F. Litvinov. – Vitebsk: VGAVM, 2009. – 24 p.
- Yatusevich, A.I. Eimeriosis nutria: monograph / A.I. Yatusevich, V.A. Forget it. – Vitebsk: OU VGAVM, 2006. – 87 p.
- Parasitology and invasive animal diseases / M.Sh. Akbaev [and others]. – M.: Kolos, 2000. – 743 p.
- Yatusevich, A.I. The pratazoin sicknesses of the rural and gaspdarchy lived. – Mn.: Urajai, 1993. – 174 p.
- Animal cryptosporidiosis (Recommendations for diagnosis, therapy and prevention). Approved by the Main Directorate of the Ministry of Agriculture and Public Administration of the Republic of Belarus on July 25, 2000. Authors: Yatusevich A.I., Savchenko V.F., Nesterovich S.G. and etc.
- Balashov, Yu. S. Blood-sucking arthropods and rickettsia / Yu. S. Balashov, A. B. Deiter. – L.: Nauka, 1973. – 251 p.
- Parasitology and invasive animal diseases / M. Sh. Ak-baev, A. A. Vodyanov, N. E. Kosminkov, etc.; edited by M. Sh. Akbaeva. – M.: Kolos, 2002. – 743 p.
- Recommendations for the fight against helminthiasis in horses / A.I. Yatusevich [and others]. – Vitebsk: VGAVM, 2008. – 15 p.
- Dubinin, V. B. Scabies mites. Biology, harm in agriculture, measures to prevent and combat them / V. B. Dubinin. -M.: Soviet Science, 1954. – 173 p.
- Agrinsky, N. I. Insects and mites that harm farm animals / N. I. Agrinsky. – M.: Selkhozizdat, 1962. – 288 p.
- Sokolova, T. V. Scabies / T. V. Sokolova, R. F. Fedorovskaya, A. B. Lange. – M.: Medicine, 1989. – 176 p.
- Yatusevich, A.I. Veterinary and medical parasitology: (Encyclopedic reference book) / A.I. Yatusevich, I.V. Rachkovskaya, V.M. Kaplich. – M.: Medical literature, 2001. – 309 p.
- Yatusevich, A.I. Eimeriosis of chickens: monograph / A.I. Yatusevich, V.N. Gisco. – Vitebsk: OU VGAVM, 2007. – 103 p.
- Karasev, N.F. Larval cestodiasis of animals / N.F. Karasev, T.G. Nikulin, N.K. Slepnev. – Mn.: Urajai, 1989. – 111 p.
- Kapustin, V.F. Atlas of helminths of farm animals. – M.: Selkhozgiz, 1953. – 139 p.
- Dubina, I.N. Methodological guidelines for diagnosing helminthiasis of carnivores: approved. GUV MASHIP RB / I.N. Club. – Vitebsk: VGAVM, 2008. – 32 p.
- Yatusevich, A.I. Helminth infections of cattle and measures to combat them under environmental pressure / A.I. Yatusevich, R.N. Protasovitskaya. – Vitebsk: VGAVM, 2010. – 160 p.
- Veterinary laboratory practice. T. 2. – M.: Selkhozizdat, 1963. – 432 p.
- Orlov, I.V. Workshop on veterinary parasitology / I.V. Orlov, N.I. Agrinsky, S.N. Nikolsky. – M.: Selkhozizdat, 1962. – 319 p.
- Practical parasitology / ed. D. V. Vinogradov-Volzhinsky. – L.: Medicine, 1977. – 304 p.
- Antiparasitic drugs for dogs and cats: educational method. allowance / A.I. Yatusevich [and others]. – Vitebsk: VGAVM, 2009. – 48 p.
- Shershen, G.G. Methodological recommendations for identifying natural foci of piroplasmosis in animals in Belarus / G.G. Shershen, N.F. Karasev. – Vitebsk: VGAVM, 2009. – 32 p.
- Midges and bovine simulidotoxicosis. / Skulovets M.V /-2007
- Parasitic diseases of horses / A.I. Yatusevich [and others]. – Mn., 1999. – 78 p.
- Kaplich, V.M. Gnus and measures to combat it in Belarus / V.M. Kaplich, A.I. Yatusevich, M.V. Skulovets. – Mn.: Urajai, 1994. – 120 p.
- Dubina, I.N. Guidelines for the diagnosis of larval cestodiasis in animals / I.N. Club. – Vitebsk: VGAVM, 2008. – 39 p.
- Diseases of agricultural animals / P.A. Krasochko [and others]; under. ed. P.A. Beautiful. – Mn.: Businessofset, 2005. – 800 p.
The structure of the parasite
The development cycle of such a parasite is reflected in the structure of the malarial plasmodium. In the early stages, the infectious agent is presented in the form of so-called schizonts. This asexual form of the parasite has the appearance of a ring, which consists of a nucleus and rough cytoplasm surrounded by a vacuole. Subsequently, the microorganism develops pseudopods. A sexually mature malarial plasmodium lacks a vacuole, and the cytoplasm acquires a reddish tint due to the absorption of hemoglobin from the host’s blood.
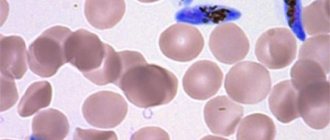
How is malarial plasmodium detected in the blood?
To detect a parasitic infection, a blood sample is examined under a microscope. The sample is taken from a person's finger in a standard way. A smear is then applied to a sterile glass slide. A specialist examines under magnification traces of the presence of malarial plasmodium in any form. The compliance of red blood cell parameters to normal is also monitored. After all, when infected by the malarial plasmodium pathogen, they change not only their shape and size, but also their shade.
General information
Adult trophozoites and schizonts resemble those of Plasmodium malariae (the pigment is in the form of individual large grains, schizonts occupy most of the red blood cells, the shape is round, pseudopodia and vacuoles are absent, the nuclei are large and irregular in shape).
Red blood cells containing Plasmodium ovale rings almost do not change in size, with the exception of red blood cells containing 2 or more rings. At the mature trophozoite stage, red blood cells enlarge, become discolored, and in some, granularity becomes visible (large, few grains of a dark red color). In approximately 1/3 of the affected red blood cells, the shape changes. In thin areas of the smear, individual red blood cells have an oval shape, which gave the name to the pathogen, and one end of the red blood cell stretches and becomes fringed. In the thick part of the smear, some red blood cells take on a round, star-shaped shape.
The morula contains 8-12 large merozoites, arranged randomly around a pile of pigment. All stages of development of the Plasmodium ovale parasite can be detected in peripheral blood.
The most characteristic differences between Plasmodium ovale and Plasmodium malariae are: the presence of several parasites in one erythrocyte with a generally small number of them in the preparation, a random arrangement of merozoites in the morula, changes in the affected erythrocytes (enlargement, discoloration, granularity, oval-elongated shape, fringe or stellation edges).
Changes in red blood cells may make it difficult to differentiate Plasmodium ovale from Plasmodium vivax. The most characteristic differences for Plasmodium ovale are the presence of several parasites in the erythrocyte with an overall small number of them in the preparation; the shape of the affected red blood cells; long-term preservation of the vacuole and ring-shaped structure in the absence of characteristic outgrowths (pseudopods); absence of young trophozoids of bizarre shape; larger sizes of nuclei and more intense coloring.
Where do mosquitoes come from?
except for the Arctic belt and deep desert. In the process of growth and development, the mosquito goes through four stages:
- egg;
- larva;
- chrysalis;
- imago ( adult
).
lakes, swamps, etc. Mosquitoes can also appear in other areas for the following reasons:
- at low temperatures, mosquitoes fall into torpor and hide ( usually in basements, dark corners, attics, etc.
); - in the warm season, mosquitoes live close to human habitation, since for many species it is humans who are the main source of food;
- mosquitoes are often found in the forest, as some species feed on the blood of other warm-blooded animals;
- Many mosquitoes are found on livestock farms, where they can breed near wells or sewers and feed on the blood of livestock.